The Silent Siege: How Invisible Superbugs Are Rewriting Nigeria’s Public Health Future
ABUJA, Nigeria – A Crisis Without a Sound It does not announce itself with sirens. There are no dramatic visuals, no mass evacuations, no single catastrophic moment that commands national attention. Yet, across Nigeria, a crisis is quietly tightening its grip—one that is dismantling modern medicine from within.
Antimicrobial resistance (AMR)—the process by which bacteria, viruses, and fungi evolve to withstand treatment—is no longer a distant scientific concern. It is here, embedded in everyday life, altering the outcome of infections that were once easily curable.
The numbers are as chilling as they are underreported. By 2050, an estimated 1.91 million deaths annually will be directly linked to bacterial AMR, a staggering rise from 1.14 million in 2021. For Nigeria, a country of over 220 million people already burdened by infectious diseases, this projection signals not just a health challenge—but a slow-burning catastrophe.
This is not a crisis of mystery. It is a crisis of behaviour, systems, and silence. Chukwu Obinna, writes.
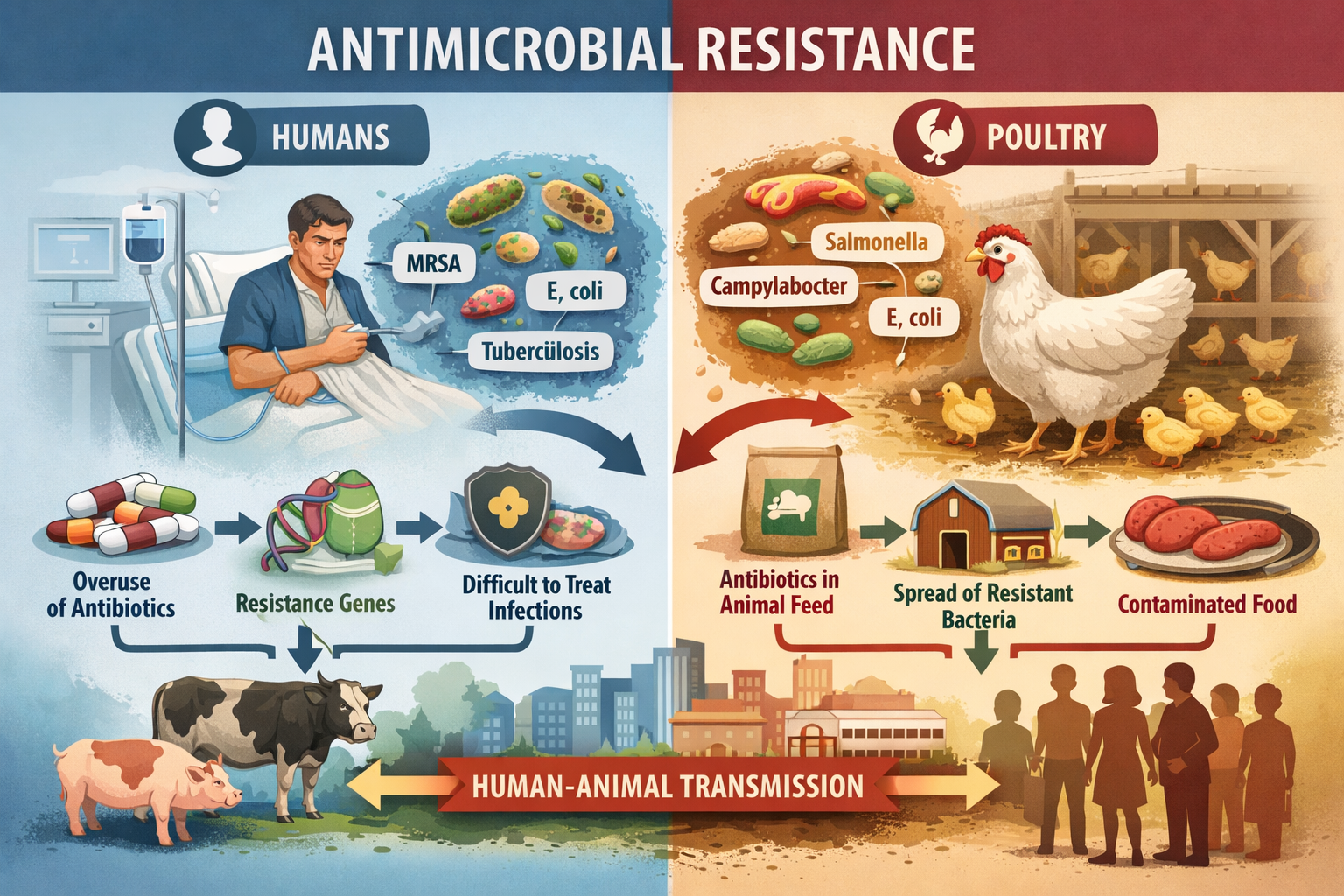
From Farm to Fork: The Invisible Pathway
The story of resistance often begins far from hospital wards—in places of routine labour and survival.
For poultry farmer Fortune Onokwuru, raising birds is both a livelihood and responsibility. His practices reflect diligence and care, particularly when it comes to vaccination and medication protocols.
“All medications and vaccines must be stopped 7 to 14 days before birds are processed for human consumption. That is the withdrawal period. It ensures the meat is safe. A lot of farmers make the mistake of administering medications too close to slaughter time.”
Onokwuru’s awareness highlights an important truth: some farmers understand food safety. Yet, this knowledge remains uneven, and crucially, incomplete.
What many do not fully grasp is that even when withdrawal periods are observed, the broader risk of antimicrobial resistance may still persist. Bacteria exposed to antibiotics—whether correctly administered or not—can evolve, survive, and eventually enter the human food chain.
What appears to farmers as normal variation in drug effectiveness may, in fact, be the early fingerprints of resistance.
Science Speaks: A Veterinarian’s Stark Warning
Dr. A.S. Sani, a practising veterinarian, offers a more clinical lens—one that bridges agriculture and human health with unsettling clarity.
Asked how long antibiotics remain in poultry, his answer is direct:
“A minimum of 14 days. That is why withdrawal periods exist.”
But the deeper concern lies beyond residue.
“Yes, of course. Absolutely. When humans consume poultry carrying antibiotic residues or resistant bacteria, they are exposed to both. Residue exposure can select for resistance in the human gut microbiome. Resistant bacteria from the bird can colonise the human digestive tract.”
The implication is profound: the farm is not separate from the clinic. It is part of the same biological system.
Dr. Sani also raises another underreported danger:
“Take penicillin, for example. Some people have severe allergies. If such residues remain in meat and are consumed, especially if not thoroughly cooked, they can trigger serious reactions.”
Yet, his perspective is not without hope. Alternatives exist—locally accessible, scientifically grounded, and underutilised.
“Natural herbal treatments can address many poultry diseases. For example, bitter leaf extract has shown effectiveness in treating coccidiosis. This is not fringe science.”
The gap, therefore, is not innovation. It is dissemination.
A Culture of Misuse
Beyond farms, the crisis deepens in communities and clinics.
Across Nigeria, antibiotics are readily available without prescription. A fever, a cough, or even fatigue often results in the purchase of drugs like amoxicillin or azithromycin—without diagnosis, without testing, and often without necessity.
This culture of self-medication is driven by accessibility, affordability, and habit.
But each misuse carries consequences.
Courses are abandoned midway. Leftover pills are shared. Antibiotics are taken for viral infections they cannot treat. Each act, seemingly insignificant, becomes part of a larger evolutionary pressure—training bacteria to survive.
In hospitals, the challenge shifts form but not severity. Limited access to diagnostic tools forces clinicians to prescribe empirically. Broad-spectrum antibiotics, meant for severe cases, become first-line treatments.
The result: a system fighting blindfolded against an adapting enemy.
Regulation in Name, Not in Practice
Nigeria is not without frameworks. Regulatory bodies exist. Policies are written. Guidelines are drafted.
Yet, enforcement remains the missing link.
Prescription-only antibiotics are sold openly in markets. Oversight is sporadic. Informal drug markets thrive alongside formal systems, often outpacing them in accessibility and affordability.
In agriculture, the absence of strict enforcement allows antibiotics to be used not just for treatment—but for growth promotion and routine prevention.
The outcome is predictable: resistant bacteria flourish across environments—farms, hospitals, and communities alike.
Even more concerning is the lack of surveillance. Without widespread laboratory capacity, resistant infections go undetected. Treatment failures are misattributed. Data remains incomplete.
A crisis that cannot be measured cannot be managed.
The Human Cost: Lives in the Balance
Behind every statistic is a story.
A child with pneumonia that no longer responds to treatment.
A surgical patient whose wound refuses to heal.
A family drained financially by prolonged hospital care.
These are not projections—they are present realities in Nigerian healthcare facilities.
What was once treatable in days now stretches into weeks, sometimes ending in loss.
The economic burden compounds the human toll. Prolonged illness leads to lost income, increased medical expenses, and, often, long-term financial instability.
AMR is not just a health crisis. It is a poverty multiplier.
Bridging the Knowledge Gap
At the heart of this crisis lies a disconnect.
The farmer who understands withdrawal periods.
The veterinarian who understands resistance.
The patient who trusts antibiotics without question.
Between them lies a gap—one that bacteria exploit relentlessly.
Closing this gap requires more than policy. It demands communication, trust, and sustained engagement.
A Future Still Within Reach
Antimicrobial resistance threatens the very foundation of modern medicine. It challenges the assumption that infections are manageable, that surgeries are safe, that treatments will work.
It directly undermines global health targets, particularly Sustainable Development Goal 3—Good Health and Well-being.
Yet, this trajectory is not fixed.
The projected 67.5 per cent increase in AMR-related deaths is not inevitable. It is a reflection of choices—made or avoided.
Nigeria stands at a crossroads.
The resistance crisis is no longer approaching. It is already here, quietly reshaping outcomes, one infection at a time.
The question is no longer whether action is needed. It is whether action will come in time.



