When the Clinic Cannot Heal: Elewura’s Struggle for Survival in Nigeria’s Failing PHC System
Elewura, Oyo State – At dawn, the first light fell not on the bustle of a working clinic, but on the haunting stillness of a health facility abandoned by the system meant to sustain it. The Elewura Primary Health Centre, once envisioned as the community’s lifeline, stood silent — its corridors empty, its doors half-fallen, its walls swallowed slowly by bush that rustled like a reminder of how nature reclaims what the government forgets.
Primary Health Centres (PHCs) form the bedrock of Nigeria’s healthcare system, designed to deliver vaccines, manage malaria, support safe deliveries and anchor rural survival. But in Elewura, that promise has withered. The centre that should protect mothers, children and the elderly has become a symbol of decay — a facility so stripped of staff, supplies and supervision that residents now survive by chance rather than care. In this report, Oluwatobi Adu enters a community forced to choose between self-medication, long treks to distant hospitals and the dangerous comfort of inaction. Elewura is more than a failing clinic — it is a national alarm bell ringing across thousands of rural communities where a weak health system is no longer merely inadequate but life-threatening.
The Clinic That Cannot Heal
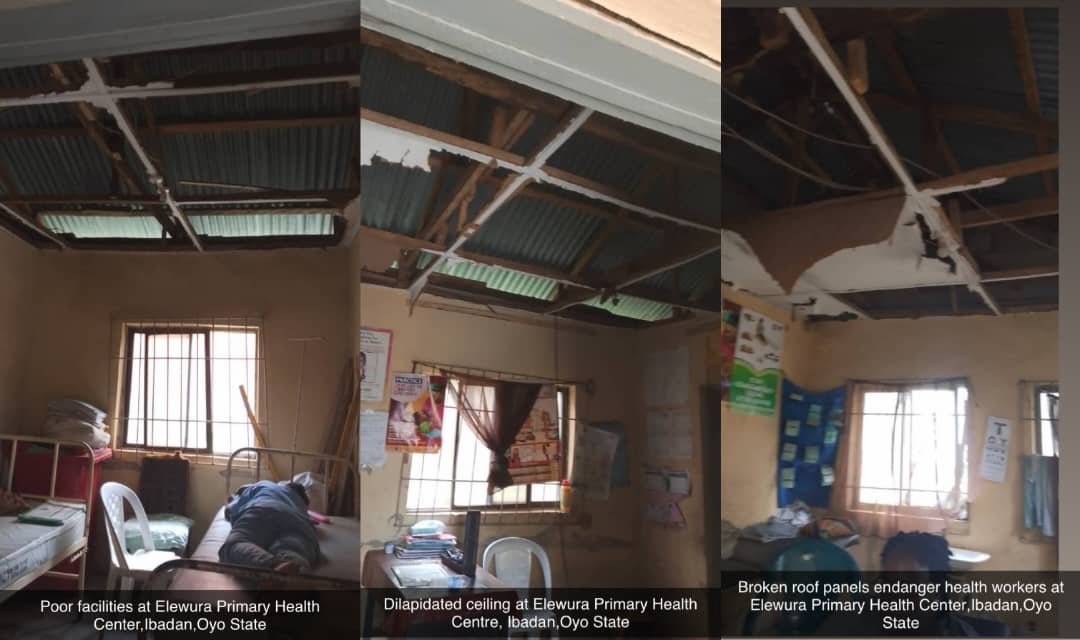
“Dilapidated building, spoiled asbestos,”
Matron Oladipupo A.A., the Officer in Charge of Elewura PHC, muttered as she pointed towards fractured walls, broken ceilings and patches of rusted roofing that leak heavily during the rains.
“The Primary Health Care is slowly turning into a bush,” she added, gesturing towards the thick vegetation swallowing the back of the building — a haven for snakes and a deterrent to expectant mothers.
For a facility expected to serve thousands across Elewura and neighbouring settlements, the structure now symbolises the national crisis: over 60% of Nigeria’s 30,000 PHCs lack basic repairs, and many rural centres receive little to no local government funding for maintenance.
Inside the PHC, the challenges multiply. There is no labour room, no family planning room, no gender-segregated wards, no water, no reliable power supply, and no laboratory — meaning even malaria tests require referrals kilometres away.
“We urgently need an antenatal room and immunisation clinic, boreholes, restoration of power supply,” she said. “We are asking the government to come to our aid… more BP apparatus, weighing scales, tiling for floors, and plastic chairs.”
Her list mirrors national shortages: Nigeria faces a deficit of more than 150,000 rural health workers, and rural PHCs operate at a 60% staffing gap, according to the National Primary Health Care Development Agency (NPHCDA).
Without a laboratory, Elewura PHC refers nearly all cases — from feverish toddlers to pregnant women — to facilities far beyond the community’s financial reach.
“Instead of referring patients, we want to treat them here,” Oladipupo explained. “But we cannot do much without the basic infrastructure.”
Voices from a Community Forced to Improvise
Mama Seun: A Mother Left with No Options
At dawn, I met Mama Seun, a mother of two who had brought her feverish child for medical attention.
“There is only one nurse, and most times they say we should go elsewhere,” she said, cradling her toddler. After receiving yet another referral she could not afford, she trekked home in frustration.
Her experience is typical in rural Nigeria, where half of all PHC consultations end without complete treatment, often forcing families into self-medication or risky traditional alternatives.
The Elder Who Gave Up on the PHC
An elderly resident, who asked not to be named, told me he no longer visits the centre at all.
“I stopped going because there is no prompt or reliable service,” he said, recalling a neighbour who suffered a breathing crisis at night but found the PHC in darkness and locked.
Nigerians are often left to fend for themselves after sunset — in a country where many emergencies, especially labour complications, occur at night.
The Human Cost — Home Births, Delayed Malaria Treatment, Preventable Deaths
Health experts describe PHC failures not in percentages but in the lives lost unnecessarily. Elewura is no exception.
A community leader revealed that at least two children in the past year died from high fever and dehydration before reaching a distant hospital.
Local birth attendants confirmed a rising number of home deliveries, many unassisted. In a state where maternal mortality remains at 262 deaths per 100,000 live births, the consequences are severe.
A public-health specialist interviewed for this report, Dr. Raliat Ogunyemi, described the situation as “a direct pathway to preventable death.”
“When PHCs collapse, maternal and child health collapses with them,” she said. “Malaria, diarrhoea, sepsis — these are easily treatable at primary level. But delay kills.”
Who Is Failing Elewura?
Local Government: The First Layer of Accountability
Under Nigerian law, the day-to-day running of PHCs belongs to the Local Government Authorities (LGAs). Yet in many states, LGAs lack autonomy or receive insufficient funds, leaving health facilities starving.
The Health Supervisor of Ibadan Southwest LGA acknowledged resource constraints.
“We have many facilities competing for limited funds,” he said, insisting that requests from Elewura would be reviewed.
State Level: Funding Gaps and Implementation Failures
Oyo State receives federal PHC funds through the Basic Health Care Provision Fund (BHCPF). But communities like Elewura say they rarely feel the impact.
A senior official at the Oyo State Primary Health Care Board, who spoke on condition of anonymity, noted staffing shortages statewide.
“Even if we approve recruitment, LGAs cannot always sustain salary payments,” the official said.
This bureaucratic tug-of-war leaves rural residents stranded.
What Must Change? The Road to Restoring Elewura PHC
Experts highlight clear reforms: Stable Funds for Infrastructure; PHCs require ring-fenced budgets to prevent diversion of funds by local officials.
Recruitment of Frontline Staff’, Community health extension workers (CHEWs), midwives and lab technicians must be posted to rural centres, Functional Laboratories; A basic diagnostic room could reduce preventable child and maternal deaths by up to 40% in rural areas, Community Oversight; Ward Development Committees (WDCs) should monitor spending, maintenance and drug supply, and Stronger State and Federal Coordination.
Experts recommend that states assume greater responsibility for PHC management, with local governments handling community mobilisation rather than finances.
When a Nation’s Hope Lies in a Village Clinic
Elewura’s Primary Health Centre is more than a building — it is a symbol of hope that has faded into disrepair. As the bush reclaims the structure and mothers cling to home remedies, one truth emerges clearly: Nigeria’s PHC system is failing those who need it most.
Matron Oladipupo’s closing plea echoes across rural Nigeria: “We are asking the government to come to our aid… through the appropriate body.”
Until that help arrives, Elewura remains a community fighting for health in a clinic that cannot heal.




well reported